Congenital Heart Defect (CHDs) are structural
abnormalities of the heart present at the time of birth of a child. CHDs are the most common cause of death due to
congenital anomalies in the developed world. Although CHD include a wide
spectrum of conditions, they can broadly be classified into critical CHD and
non-critical CHD. Critical CHDs are those defects where failure to identify the
condition within the first month after birth could potentially result in death
or a significant disability. The critical CHDs include Pulmonary atresia, Severe
Pulmonary stenosis or atresia, Hypoplastic left heart syndrome, Aortic
stenosis, Transposition of Great arteries, Obstructed total anomalous pulmonary
venous drainage and Severe coarctation. Timely diagnosis is critical to the
effective treatment forcongenital heart defects.
However, the clinical
recognition of CHD in the newborn period is often challenging. This is because
the symptoms of CHDs are similar to other common newborn conditions such as
persistent pulmonary hypertension of the newborn, sepsis (bloodstream
infections) and lung infections. The situation is further compounded in our
country where pediatric cardiac centers exist as separate silos away from
secondary and tertiary care pediatric hospitals. As a result of this, pediatricians
or pediatric residents are not adequately trained to detect CHD in the neonatal
period. Hence it is not unusual for children with critical CHD to go on without
a diagnosis, leading to the delayed Treatment for Congenital Heart Defects.
There are two
powerful tools to detect critical Congenital Heart Defect within an appropriate
time frame. The first of these, a prenatal fetal echocardiogram helps in prenatally diagnosed congenital heart disease (link to
RP-2-730.pmd
(genesis-foundation.net) . This is obtained by an ultrasound examination of the baby’s heart
while the baby is still in the mother’s womb. The study is ideally performed
between 18-22 weeks of pregnancy but can potentially be performed at any point
till the 40 weeks of pregnancy. Ultrasound is a safe, widely available and
relatively inexpensive tool with the potential to detect more than 80% of
critical CHD when performed by someone with adequate training (a pediatric cardiologist
or a fetal medicine specialist with special training in fetal
echocardiography). If a critical CHD is diagnosed prenatally, it allows the
family to take an informed decision about further management of the baby. Thus,
the family can plan for Treatment
for Congenital Heart Defects in a better way.
The state of Kerala
has embraced prenatal echocardiography as a key component of their flag ship
“HRIDYAM” program– the first state sponsored universal insurance program for
congenital heart disease in the country. This involved devising a simple
protocol for training radiologists, obstetricians and sonologists to identify
CHD. Training programs were conducted in all parts of the state by experienced
pediatric cardiologists and fetal medicine specialists. The training focused on
three simple views which could easily be obtained by those performing obstetric
ultrasound. An abnormality in one or more of these views could raise the
suspicion of a critical CHD and enable the operator to refer the mother to an
advanced facility where an accurate diagnosis and postnatal management pathway
can be charted.
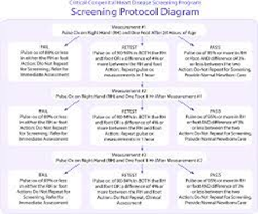
The second modality available for timely diagnosis of
critical CHD is pulse oximetry screening (POS) of the neonate in the first
24-48 hours of life. This involves placing a pulse oximeter, a device used to
measure the oxygen level in the blood, on the baby’s foot or hand. An oxygen
level, termed as SpO2 (or oxygen saturation), of greater than 97% detected in
the lower limbs rules out almost all critical CHD. An oxygen saturation of less
than 95% or a difference in saturation of greater than 2% between the upper and
lower limbs should prompt referral for pediatric cardiac evaluation. Universally,
POS has been shown to be an effective diagnostic tool for early detection of
CHD. It can be performed very easily by a trained para-medical personnel and
costs involves in buying the equipment and training staff are meagre compared
to the rich rewards it could yield. A diagnosis, can then enable the doctors
and families to plan the treatment
for congenital heart defects.

Although protocols
for POS exist and have been strongly recommended by both the governmental
departments as well as professional bodies, implementation continues to remain
inconsistent even in tertiary care institutes. Challenges include substandard
pulse oximeters, improper training of staff and lack of manpower. A more
important challenge is the lack of a mandate to perform POS. In the absence of
a mandate, it is often challenging to procure equipment and train personnel
References:
1. Saxena A. Congenital heart disease in
India: a status report. Indian Pediatr. 2018;55:1075–82.
2.
Vaidyanathan B, Sathish G,
Mohanan ST, Sundaram KR, Warrier KK, Kumar RK. Clinical screening for
congenital heart disease at birth: a prospective study in a community hospital
in Kerala. Indian Pediatr. 2011;48:25–30.
3.
Mahle WT, Newburger JW, Matherne
GP, et al. Role of pulse oximetry in examining newborns for congenital heart
disease: a scientific statement from the AHA and AAP. Pediatrics. 2009;124:823–36.
4.
Bakiler AR, Ozer EA, Kanik A,
Kanit H, Aktas FN. Accuracy of prenatal diagnosis of congenital heart disease
with fetal echocardiography. Fetal Diagn Ther. 2007;22:241–4.





Comments
Post a Comment